Sign up to our newsletter Subscribe
Challenges and Solutions for Budget Impact Analysis of Gene Therapies

In a commentary piece recently published in Applied Health Economics and Health Policy, OHE authors discuss how the misalignment in interpretations of the term ‘unmet medical need’ by different stakeholders has led to insufficient incentives for development in areas with…
In a commentary piece recently published in Applied Health Economics and Health Policy, OHE authors discuss how the misalignment in interpretations of the term ‘unmet medical need’ by different stakeholders has led to insufficient incentives for development in areas with urgent, genuine need, and propose a new framework for developing a more consistent understanding of UMN that will increase innovation.
In a commentary piece recently published in Applied Health Economics and Health Policy, OHE authors discuss how the misalignment in interpretations of the term ‘unmet medical need’ by different stakeholders has led to insufficient incentives for development in areas with urgent, genuine need, and propose a new framework for developing a more consistent understanding of UMN that will increase innovation.
The term ‘unmet medical need’ (UMN) is often used to signal special priority for treatments that address pressing medical needs. However, the understanding of UMN is often context-specific, leading to a lack of alignment in the way it is interpreted by different stakeholders (including public research funders, health regulators, and health technology assessment (HTA) agencies) in terms of priority-setting. A review by Vremen et al. (2019) found 16 different operational definitions of UMN, many of which differed in substantive respects. A shared understanding of what constitutes an UMN is critical to providing a consistent and reliable signal to innovators, thus such misalignment has arguably been a barrier to innovation in areas of genuine medical need.
At its essence, UMN is meant to distinguish more urgent societal health needs from those that are less urgent. As a first step in addressing this misalignment, we propose a conceptual framework based on principles of distributive justice as a means of developing a shared understanding of objectives around UMN. Central to this approach is recognising that stakeholders can identify a set of rationale, based on a shared vision of ‘fairness’, upon which a set of principles for priority-setting might be agreed.
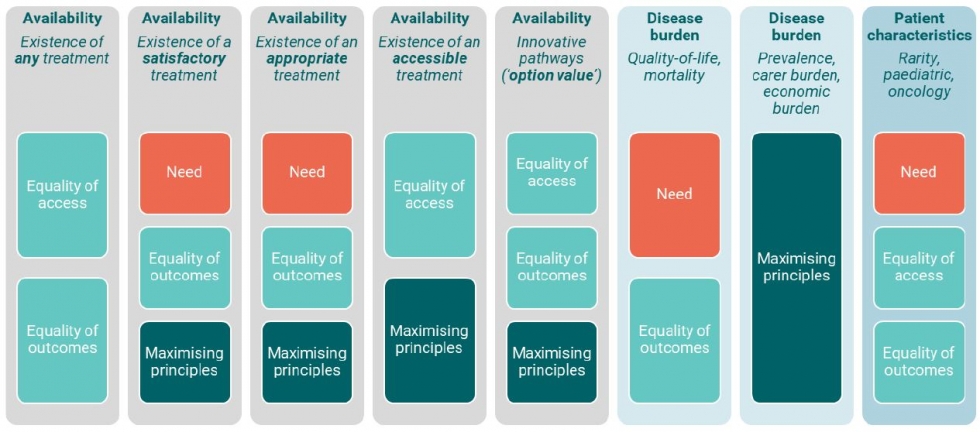
Figure 1 below presents an illustration of the way by which various principles – e.g. concern for need, inequality, and wellbeing maximisation – relate to the various elements of UMN described in the review by Vreman et al. (2019) – including aspects of availability, disease burden, and patient characteristics. This is not to imply that these are the only principles relevant to understanding UMN, and different readers may see different principles reflected in different elements of UMN. These are only intended to serve as a starting point for discussion. Any process of reconceptualising UMN must be stakeholder-led to achieve consensus over identified principles.
Figure 1. Illustration of key principles within elements of unmet medical need
A key challenge here is that these principles represent often conflicting concerns (e.g. the incompatible objective of simultaneously equalising and maximising outcomes. Hence, trade-offs must be made between objectives, and different stakeholders may assign a different degree of importance to each objective. Discussing differing priorities and objectives at the level of principles rather than quantitative criteria (e.g. ‘a need is only ‘unmet’ if there are no available alternatives’) allows stakeholders to consider these trade-offs in a more constructed manner than is possible under the often binary and disconnected criteria by which UMNs are currently understood.
Agreeing on a principles-based framework will not in itself provide an operational definition of UMN However, it is an important initial step towards reconceptualising UMN to improve alignment between stakeholders, and in turn, providing a more reliable and consistent signal to innovators.
References
Vreman RA, Heikkinen I, Schuurman A, et al. Unmet medical need: an introduction to deinitions and stakeholder perceptions. Value Health. 2019; 22:1275–82. https://doi.org/10.1016/j.jval.2019.07.007
Citation
Zhang, K., Kumar, G. & Skedgel, C. Towards a New Understanding of Unmet Medical Need. Appl Health Econ Health Policy (2021). https://doi.org/10.1007/s40258-021-00655-3










